Can You Be Certain?
December 15, 2025
You are asked for your opinion on this electrocardiogram (ECG). No history is available. Can you be certain of your diagnosis?
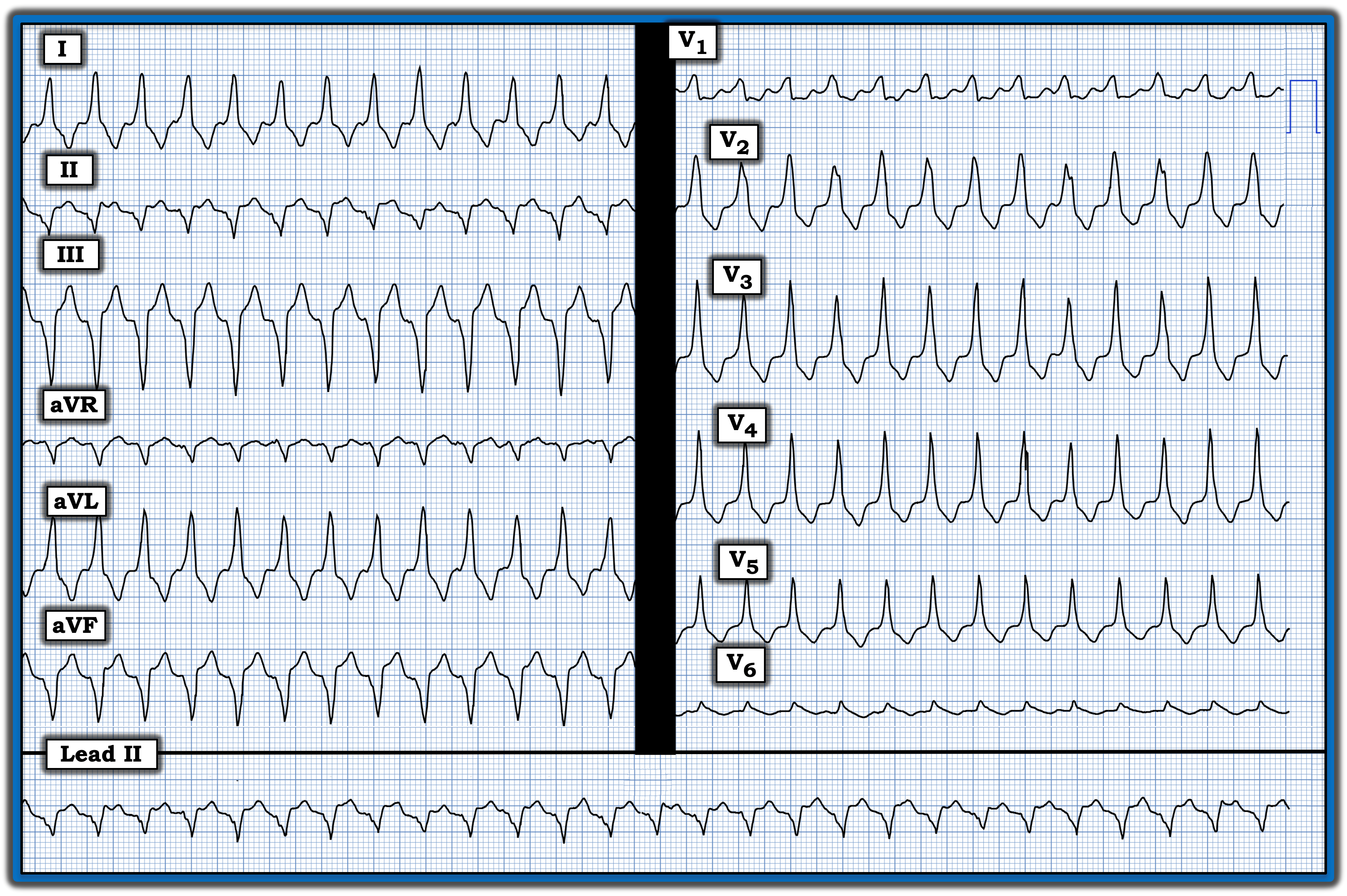
Interpretation: The rhythm in today’s ECG is a regular wide-complex tachycardia (WCT). The principal differential diagnosis is between ventricular tachycardia (VT) and some form of supraventricular tachycardia (SVT) with either preexisting bundle branch block or QRS widening as a result of aberrant conduction because of the rapid rate. Other less common entities include Wolff-Parkinson-White- (WPW)-related arrhythmias and some form of toxicity, such as hyperkalemia, that might result in QRS widening without P waves at a rapid rate. That said, most of the time, our differential diagnosis is between VT vs. some form of SVT rhythm.
- The ventricular rate of today’s rhythm is between 160-170 beats/minute.
- There is no clear sign of atrial activity.
Knowing nothing more than that the rhythm is a regular WCT, it is helpful to remember that statistical likelihood of VT is at least 80%, even before you look at the tracing.
- This statistical probability could be refined (and would approach 90%) if the patient was middle-aged or older — and if the patient was known to have underlying heart disease.
Other easy-to-use features that can improve the accuracy of your diagnosis include assessment of the frontal plane axis and QRS morphology of the WCT rhythm. In today’s case:
- There is extreme frontal plane axis deviation because the QRS complex is entirely negative in each of the inferior leads. This finding greatly increases the likelihood of VT.
- QRS morphology does not resemble any known form of conduction defect. Although the limb leads are consistent with left bundle branch block, the all positive R wave in lead V1 is not. Instead, the positive R wave in lead V1 suggests right bundle branch block, but the lack of lateral lead S waves rules out this possibility.
- There is “global positivity” in the chest leads (i.e., monophasic R waves are seen in all six chest leads).
Impression: The combination of the previously mentioned features makes it almost certain that today’s WCT rhythm is VT. The only other possibility would be if the patient had a highly distorted baseline tracing from severe underlying heart disease. This is highly unlikely. Today’s rhythm needs to be treated as VT until proven otherwise.
NOTE: For more information about this case, visit https://tinyurl.com/KG-Blog-468
Ken Grauer, MD, is Professor Emeritus in Family Medicine, College of Medicine, University of Florida, Gainesville.