Peaked T Waves
Key takeaways
- Peaked T waves are a pattern, not a diagnosis. Their significance depends on morphology, lead distribution, associated ECG changes, and patient context.
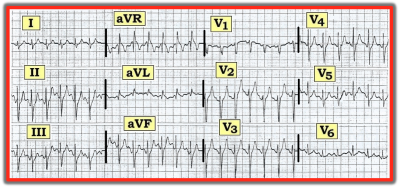
- Hyperkalemia classically causes diffuse, narrow, symmetric, tented T waves and may progress to PR prolongation, P-wave loss, QRS widening, and sine-wave morphology.
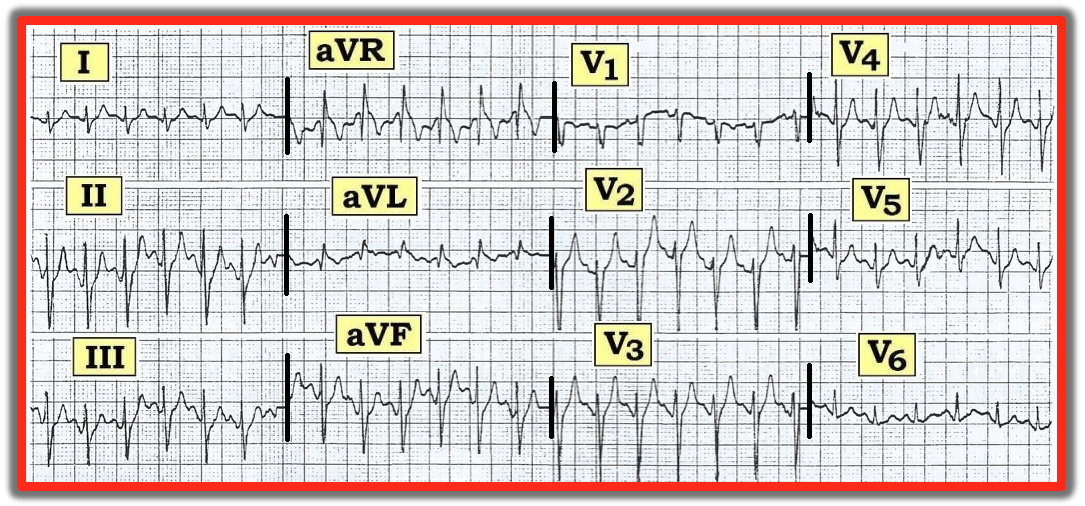
- Hyperacute ischemic T waves are usually broader-based and localized rather than diffuse.
- A normal ECG does not exclude clinically important hyperkalemia.
- Serial ECGs, laboratory correlation, and clinical context are essential for accurate interpretation.
Peaked T waves are a classic electrocardiogram (ECG) clue, but they are not a diagnosis by themselves. In practice, the finding matters because it can be an early sign of hyperkalemia, a marker of acute coronary occlusion, or a normal-variant appearance in select patients. The clinical task is not simply to recognize a tall T wave.
It is to determine whether the T wave is narrow and tented, broad and hyperacute, or simply prominent but benign in context.
What are peaked T waves?
The T wave reflects ventricular repolarization. A normal T wave is usually asymmetric, with a more gradual upstroke and a steeper downstroke. When clinicians describe a “peaked” T wave, they usually mean a T wave that is unusually tall, pointed, and often more symmetric than normal.
The highest-yield distinction is morphology: hyperkalemic T waves are classically tall, narrow, and tented, whereas ischemic hyperacute T waves are typically broad-based and bulky rather than needle-like.
Peaked T waves on ECG
On ECG, true pathologic peaked T waves are interpreted by combining waveform shape, lead distribution, interval changes, and clinical context. Diffuse, narrow, symmetric T-wave peaking across multiple leads raises concern for hyperkalemia, especially when accompanied by PR prolongation, P-wave flattening, or QRS widening. By contrast, localized tall T waves in an anatomic territory, particularly with evolving ST-segment change, should raise concern for acute coronary occlusion.
A practical bedside approach is to ask four questions:
- Are the T waves diffuse or localized?
- Are they narrow and tented or broad and bulky?
- Are there accompanying conduction abnormalities?
- Does the patient’s history fit hyperkalemia, ischemia, or a benign variant?
Peaked T waves and hyperkalemia
Hyperkalemia is the diagnosis most clinicians associate with peaked T waves, and for good reason. Early ECG changes in hyperkalemia often include tall, symmetric, peaked T waves caused by shortened ventricular repolarization. As potassium rises further, the ECG may progress to PR prolongation, P-wave flattening or disappearance, QRS widening, bradyarrhythmias, a sine-wave pattern, ventricular fibrillation, or asystole.
That said, peaked T waves are neither perfectly sensitive nor perfectly specific for clinically important hyperkalemia. Some patients with substantial potassium elevation have minimal ECG change, while others with chronic kidney disease or mixed electrolyte disturbances may show atypical patterns. A normal ECG does not exclude dangerous hyperkalemia.
Clinically, the combination of diffuse narrow-based T-wave peaking plus a compatible setting — chronic kidney disease, acute kidney injury, potassium-retaining medications, tissue breakdown, or metabolic acidosis — should trigger immediate potassium confirmation and treatment planning, not watchful waiting.
Causes of peaked T waves
Hyperkalemia is the most important cause, but it is not the only one. Here are some key differentials.
Hyperkalemia
This is the classic cause. T waves are typically tall, narrow, symmetric, and diffuse. As severity increases, conduction delay becomes more apparent.
Hyperacute ischemic T waves
In acute coronary occlusion, early T waves may become tall and symmetric before clear ST elevation appears. Unlike hyperkalemic T waves, these are usually broader based, often localized to a vascular territory, and tend to evolve dynamically on serial ECGs.
Normal variant or physiologic prominence
Some healthy patients, especially younger adults, can have relatively prominent precordial T waves without pathology. In these cases, the T waves generally lack the classic tented morphology of hyperkalemia, the ECG is otherwise stable, and the clinical picture is reassuring.
Early repolarization
Early repolarization can produce prominent T waves, usually with characteristic J-point elevation and concave ST-segment morphology. These T waves are typically not the narrow, sharply pointed pattern associated with hyperkalemia.
Meanings and interpretations
The meaning of peaked T waves depends on context, not amplitude alone. A single prominent T wave in a young, asymptomatic person is very different from new diffuse tented T waves in a patient with missed dialysis. Similarly, broad hyperacute T waves in a patient with chest pain should not be mislabeled as hyperkalemia solely because they are tall.
In day-to-day interpretation, the most useful distinctions are these:
- Diffuse + narrow + symmetric + conduction slowing favors hyperkalemia.
- Localized + broad-based + evolving ST change favors acute coronary occlusion.
- Stable tracing + no symptoms + reassuring history may represent a normal variant.
Normal vs. abnormal peaked T waves
Not every tall T wave is abnormal. Normal T waves are usually asymmetric, and prominence can vary by lead, age, body habitus, and baseline repolarization pattern. What makes a T wave concerning is not just height, but the overall pattern: a pointed, symmetric, tent-like contour, diffuse distribution, and associated interval or rhythm abnormalities.
A useful clinical shorthand is:
More likely normal or benign
- Stable ECG appearance compared with prior tracing
- No concerning symptoms
- No renal failure, potassium-retaining medications, or acidosis
- Prominent but not sharply tented T-wave shape
More likely abnormal
- New diffuse peaked T waves
- Narrow, symmetric, tented morphology
- PR prolongation, P-wave flattening, bradycardia, or QRS widening
- Compatible clinical setting, such as kidney disease, missed dialysis, ACE inhibitor use, potassium-sparing diuretic use, or chest pain suggestive of ischemia
Common pitfalls
One common error is assuming that peaked T waves always equal hyperkalemia. They do not. Acute ischemia can also produce tall symmetric T waves, but those T waves are usually broader and regional rather than diffuse.
Another pitfall is assuming that severe hyperkalemia must produce dramatic T-wave peaking. In reality, dangerous hyperkalemia may present without classic ECG findings, particularly in patients with chronic kidney disease or complex metabolic disturbances.
A third mistake is focusing on T-wave height alone. Morphology, distribution, intervals, serial change, and the bedside story are usually more informative than amplitude in isolation.
When peaked T waves require urgent action
Peaked T waves warrant urgent evaluation when they are new, diffuse, associated with bradycardia or QRS widening, or seen in a patient with known kidney dysfunction, suspected hyperkalemia, or acute ischemic symptoms. In those settings, clinicians should rapidly correlate the ECG with potassium measurement, medication review, renal function, and the overall clinical picture. Hyperkalemia with ECG changes is a medical emergency because progression to malignant arrhythmia can be rapid.
Frequently Asked Questions
Are peaked T waves always caused by hyperkalemia?
No. Hyperkalemia is the classic cause, but acute coronary occlusion, early repolarization, and normal variation can also produce prominent T waves. The distinction depends on shape, distribution, associated findings, and the clinical setting.
What do hyperkalemic peaked T waves look like?
They are typically tall, narrow, pointed, and symmetric, often appearing diffusely rather than in a single vascular territory. As hyperkalemia worsens, PR prolongation, P-wave flattening, and QRS widening may appear.
How are hyperacute T waves different from hyperkalemic T waves?
Hyperacute ischemic T waves are generally broad-based and localized to affected leads. Hyperkalemic T waves are classically narrow-based, tented, and diffuse.
Can severe hyperkalemia occur without peaked T waves?
Yes. Some patients with significant hyperkalemia have few or no classic ECG abnormalities, so clinicians should not use a normal ECG to rule it out.
When should clinicians worry most about peaked T waves?
Concern should be highest when the finding is new, diffuse, accompanied by conduction abnormalities, or present in a patient with renal dysfunction, potassium-retaining medications, missed dialysis, weakness, bradycardia, or chest pain.
Are peaked T waves ever normal?
Some individuals have prominent T waves as a baseline variant, especially in precordial leads. A benign pattern is more likely when the morphology is not sharply tented, symptoms are absent, and the tracing is stable over time.