
The History Matters!
November 15, 2025
By Ken Grauer, MD
How would you interpret today’s 12-lead electrocardiogram (ECG) and long lead V1 rhythm strip if the history was that of an older adult with known coronary disease? Would your interpretation change if, instead, the patient was a younger adult with a known history of severe congenital heart disease (CHD), having been operated on a number of times as a child?
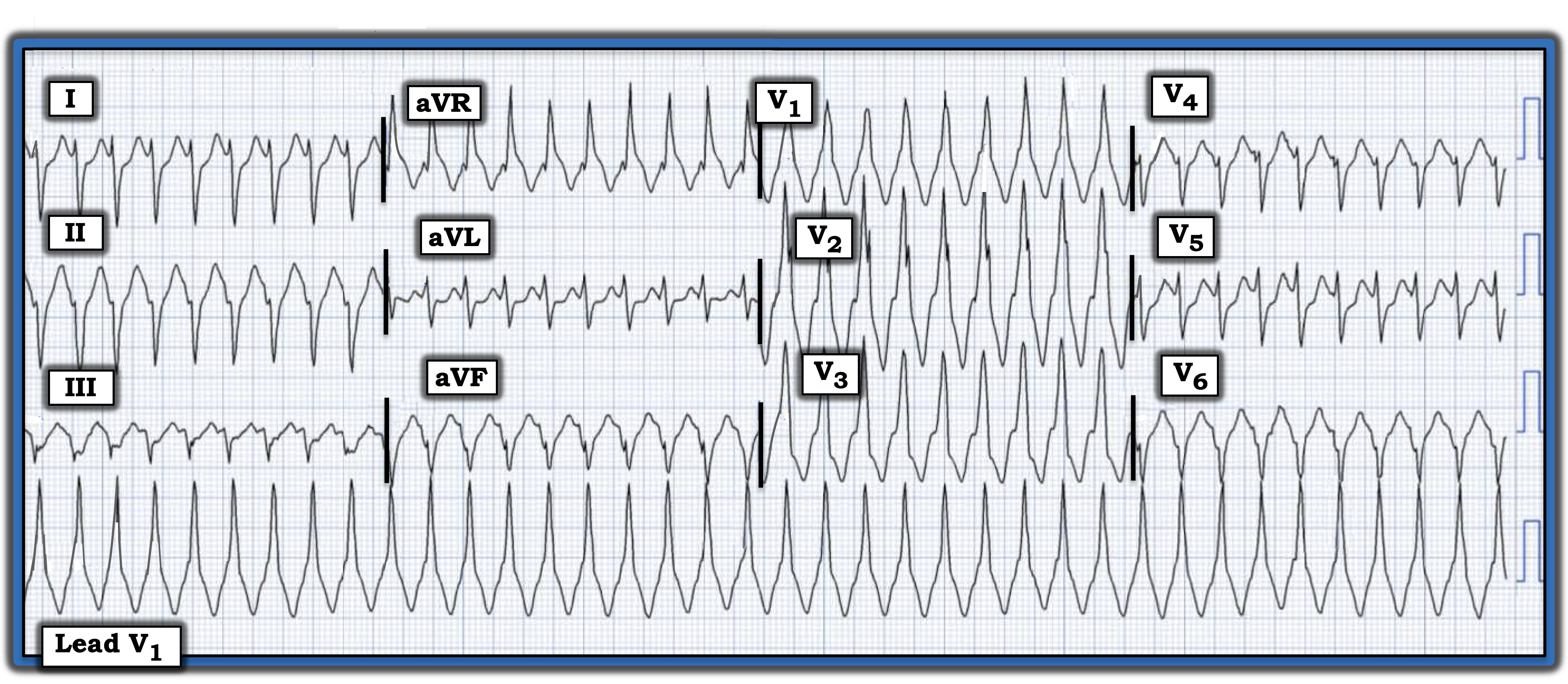
Interpretation: The ECG in the figure represents a regular wide-complex tachycardia (WCT) at ~225 beats/minute, without clear sign of atrial activity.
- If the history in today’s case was of an older adult with known coronary disease, I would estimate a greater than 95% likelihood that this rhythm was ventricular tachycardia (VT). Statistically, at least 90% of regular WCT rhythms without atrial activity in adults with known coronary disease will turn out to be VT. Also, there is “extreme” axis deviation in the frontal plane (predominantly negative QRS complexes in all three standard leads — leads I, II, and III), with the QRS essentially all negative in lead aVF.
Meanwhile, the QRS is all positive in lead aVR and essentially all negative in lateral chest lead V6. Lastly, the QRS morphology in the figure does not resemble any known form of bundle branch block (i.e., the indeterminate frontal plane axis and essentially all negative QRS in lead V6 are against right bundle branch block conduction [RBBB]).
On the other hand, if this is a younger adult patient who is a CHD survivor, VT is a far less certain cause.
- By definition, the history of severe CHD necessitating a series of operations tells us that this patient’s baseline ECG is likely to be very abnormal!
- Several leads in this tracing manifest a surprisingly narrow initial QRS deflection (e.g., leads I, aVL, and V5). This suggests rapid initial depolarization, which is consistent with supraventricular reentry rhythms (such as atrioventricular nodal reentrant tachycardia and atrioventricular reciprocating tachycardia) in which initial depolarization is rapid because it traverses the normal atrioventricular conduction system.
Follow-up: It turns out that today’s rhythm was supraventricular, with the patient having a very abnormal prior ECG that showed RBBB/left anterior hemiblock and a very similar QRS morphology during sinus rhythm.
For more information about this case, visit https://tinyurl.com/KG-Blog-455.
Ken Grauer, MD, is Professor Emeritus in Family Medicine, College of Medicine, University of Florida, Gainesville.