A Run of Aberrant AFib?
June 15, 2024
By Ken Grauer, MD
Professor Emeritus in Family Medicine, University of Florida
The patient whose electrocardiogram (ECG) appears in the figure is a previously healthy man who presented to the emergency department because of acute dyspnea. What is the cause of the run of wide beats?
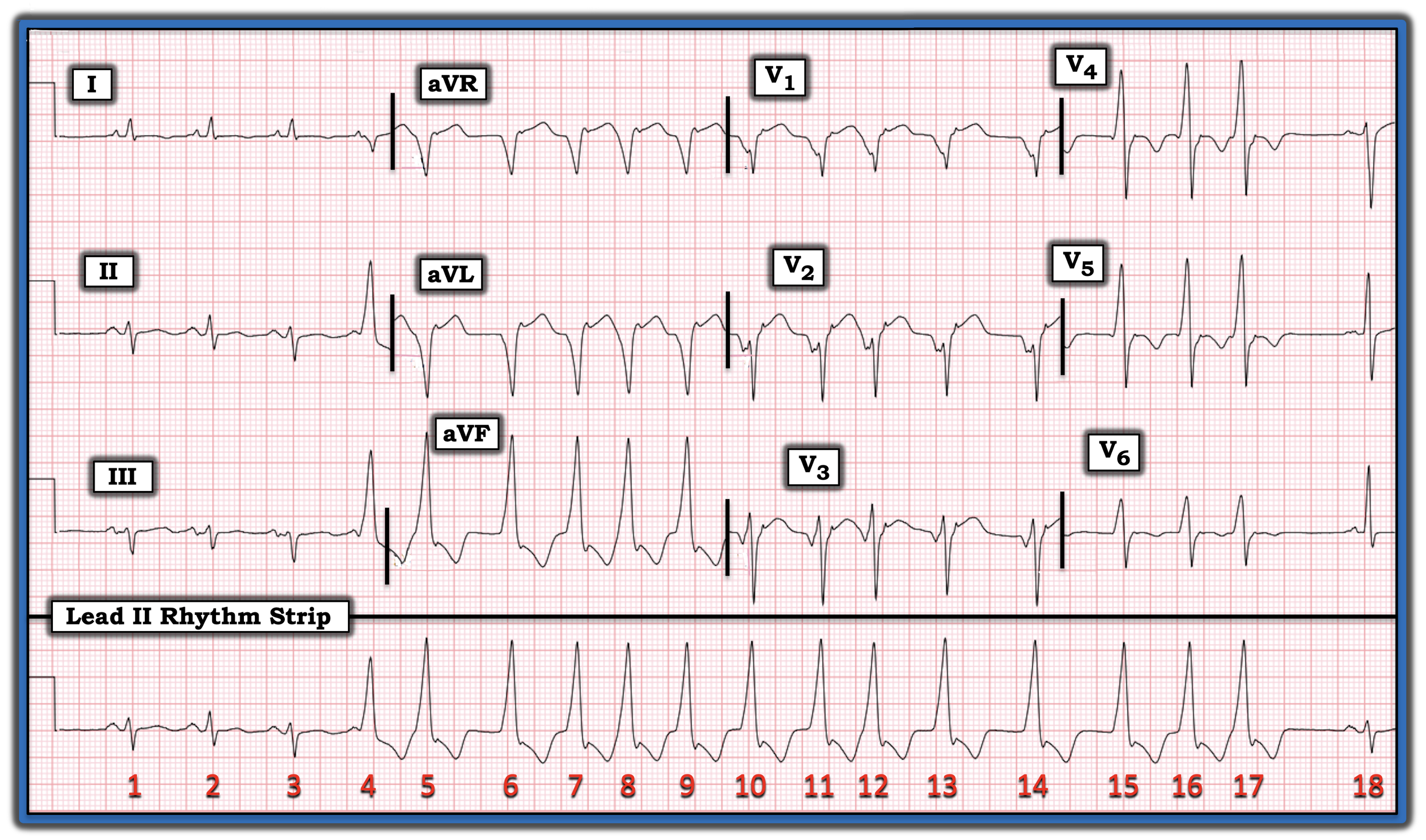
Interpretation: As always, I favor at least a brief look at the simultaneously recorded long lead rhythm strip before shifting my attention to the 12-lead ECG.
This tip is especially helpful in today’s case because assessment of ST-T wave morphology is less reliable in leads in which the QRS complex is wide.
- As a result — assessment of ST-T wave morphology will be reliable only for beats 1, 2, and 3 in simultaneously recorded leads I, II, and III. These leads show three initial beats of sinus rhythm with marked left axis deviation (consistent with left anterior hemiblock), and nonspecific ST-T wave changes — but do not suggest anything acute.
- The final QRS complex in today’s ECG is a narrow, sinus-conducted beat ( = beat #18), but the tracing ends before we see the ST-T wave of this last beat.
Regarding today’s rhythm — after three narrow, sinus-conducted beats — the QRS complex widens, and remains wide from beat #4 until beat #17.
- Note that the rhythm is irregularly irregular during this run of 14 wide beats (from beat #4 until beat #17).
- Although the irregular irregularity of these 14 wide beats suggest atrial fibrillation, this is not the etiology because the first wide beat (beat #4) has a relatively long coupling interval, such that there is no reason for sudden development of aberrant conduction (which usually is seen in association with a short coupling interval) and beat #4 is a fusion beat!
- Note that the beginning of an on-time sinus P wave is seen just before the beginning of the QRS complex of beat #4. The PR interval of beat #4 is, therefore, too short to conduct normally.
- Note also that R wave amplitude of beat #4 is slightly shorter than R wave amplitude of the 13 wide beats that follow. This is not by chance — but instead reflects that there is “fusion” between beginning conduction of the on-time sinus P wave before beat #4 — and the first beat in this 14-beat run of ventricular tachycardia VT!
- Recognition of the fusion beat proves that the run of wide beats in this tracing is VT. And although monomorphic VT usually is a regular rhythm — today’s case shows that it may sometimes be irregular!
Note: For more information about this case, visit https://tinyurl.com/KG-Blog-417.