
Subtle but Real?
March 15, 2025
By Ken Grauer, MD
The electrocardiogram (ECG) in the figure was obtained from an older man with intermittent chest pain that has awakened him from sleep. How would you interpret this ECG? Should you activate the cath lab?
Interpretation: The history we are given is brief. That said, this history is definitely of concern because the patient experienced the sudden onset of chest pain severe enough to awaken him from sleep. Although some of the ECG changes on this tracing are subtle — they are sufficiently distinct, and present in enough leads to strongly suggest a recent (if not ongoing) acute cardiac event.
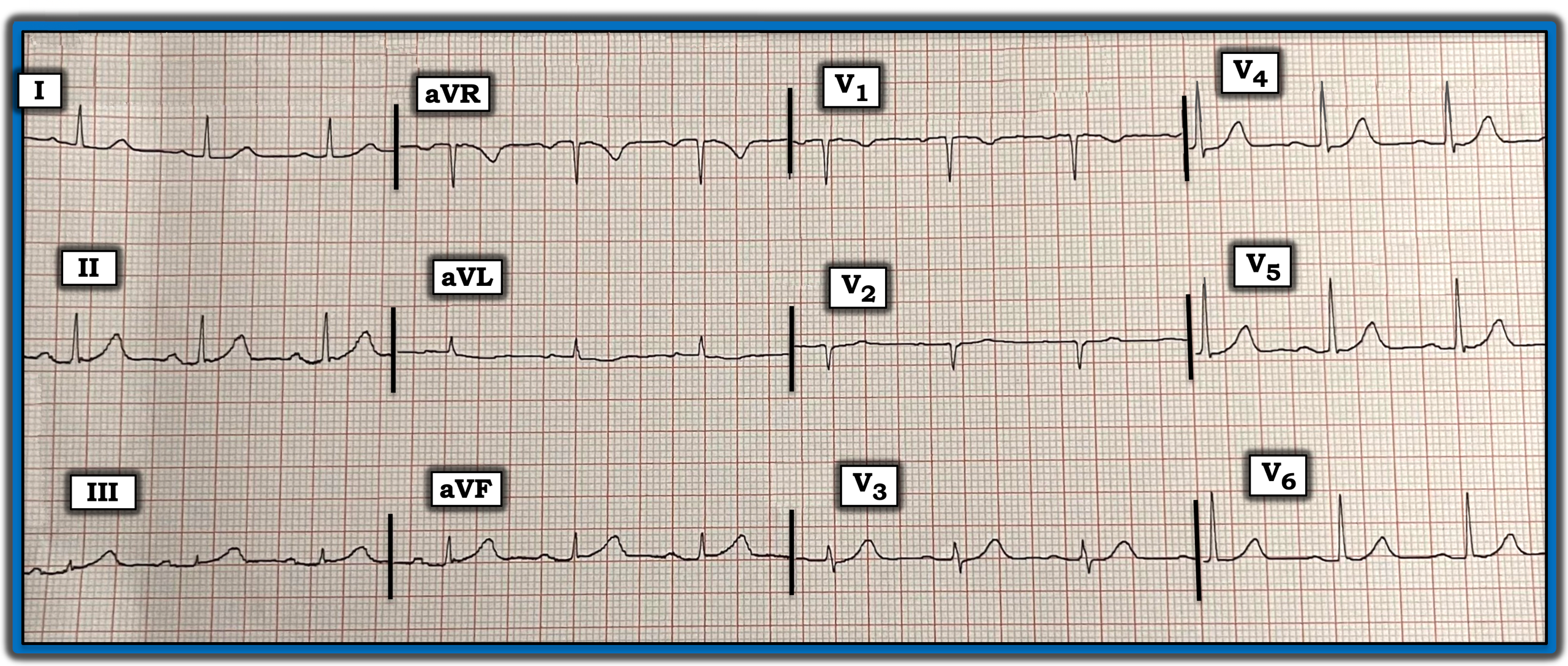
The inferior leads immediately catch the eye:
- The most remarkable lead is lead III. In a patient with new chest pain, the T wave in lead III clearly is hyperacute — it is “fatter” at its peak and both taller and wider at its base than expected, considering how tiny the amplitude of the QRS in this lead is.
- The T wave in neighboring lead aVF also is hyperacute. It is nearly as tall as the small R wave in this lead and much “fatter” at its peak and wider at its base than expected.
- In the context of these two definitely abnormal inferior leads, I interpreted the more subtle T wave prominence in the third inferior lead (lead II) also as being more prominent than expected.
- Supporting evidence that these inferior lead T wave changes are acute is the presence of subtle-but-real reciprocal ST-T wave depression in lead aVL.
Because of its common blood supply, infarction of the inferior wall often is accompanied by ECG evidence of posterior infarction. This typically manifests as chest lead ST-T wave changes that are maximal in leads V2 through to V4.
- Normally, leads V2 and V3 manifest a slight amount of gently upsloping J-point ST elevation. This clearly is lost in lead V2, which shows a flat ST segment and loss of the normally upright T wave that usually is seen in this lead.
- Lead V3 is even more obviously abnormal in that it shows a flat ST segment and an obviously hyperacute T wave that is taller and clearly more voluminous than expected, with respect to the small amplitude QRS in this lead.
Impression: In an older man awakened from sleep by new-onset severe chest pain, the summation of the above ST-T wave changes strongly suggest recent and/or ongoing acute infero-postero infarction. Prompt cardiac catheterization is indicated — with probable need for percutaneous coronary intervention.
Note: For more information about this case, visit https://tinyurl.com/KG-Blog-426.